
Last week, my wife and I welcomed our first child into the world. It is difficult to imagine a more profound testimony to design than the delivery of a fully developed baby that, only nine months ago, was a single cell. The degree of regulatory control and informational complexity of the process that drives embryonic development is far beyond human comprehension. Few biological phenomena are as gripping and awe-inspiring as the process of reproduction and the development of a baby in utero. The signature of design here is unmistakable, for so much of the process — from conception to delivery — depends on foresight and planning.
Up until birth when our son took his first breath, he was fully dependent for his oxygen supply upon the flow of maternal blood through the placenta and umbilical cord. Following his delivery, I was handed a pair of scissors by the midwife and invited to cut the umbilical cord. By doing so, I was severing our son’s connection to his mother’s blood and thus to his supply of oxygen. The placenta was also delivered momentarily after his birth, having served its task. As he made the transition from dependence on the placenta and umbilical cord for gas exchange to breathing outside of the uterus, he needed oxygen — and quickly. Moreover, the flow of blood in the umbilical vein must immediately be turned off. The changes that have to take place in the baby’s lungs and heart must happen rapidly, or the consequence will be fatal. Here, I will review the differences between the circulatory systems of the fetus and infant, describe the changes that must rapidly take place, and offer an evaluation of the respective merits of evolution and design. The information that follows is well-established and can be found in any decent textbook on anatomy and physiology. This material is also covered by medical physician and president of the UK Centre for Intelligent Design Dr. David Galloway, in his book, Design Dissected — Is the Design Real? A Clinical Look at Life’s Complexity, Design, and Ultimate Causation, a book that I highly recommend. [1] Dr. Galloway also discusses it in this episode of the ID the Future podcast.
The Circulatory System After Birth
After birth, the circulatory system follows a recognized pathway, memorized by every biomedical student. If this is unfamiliar territory, than I suggest consulting the following diagram of the heart as you read.
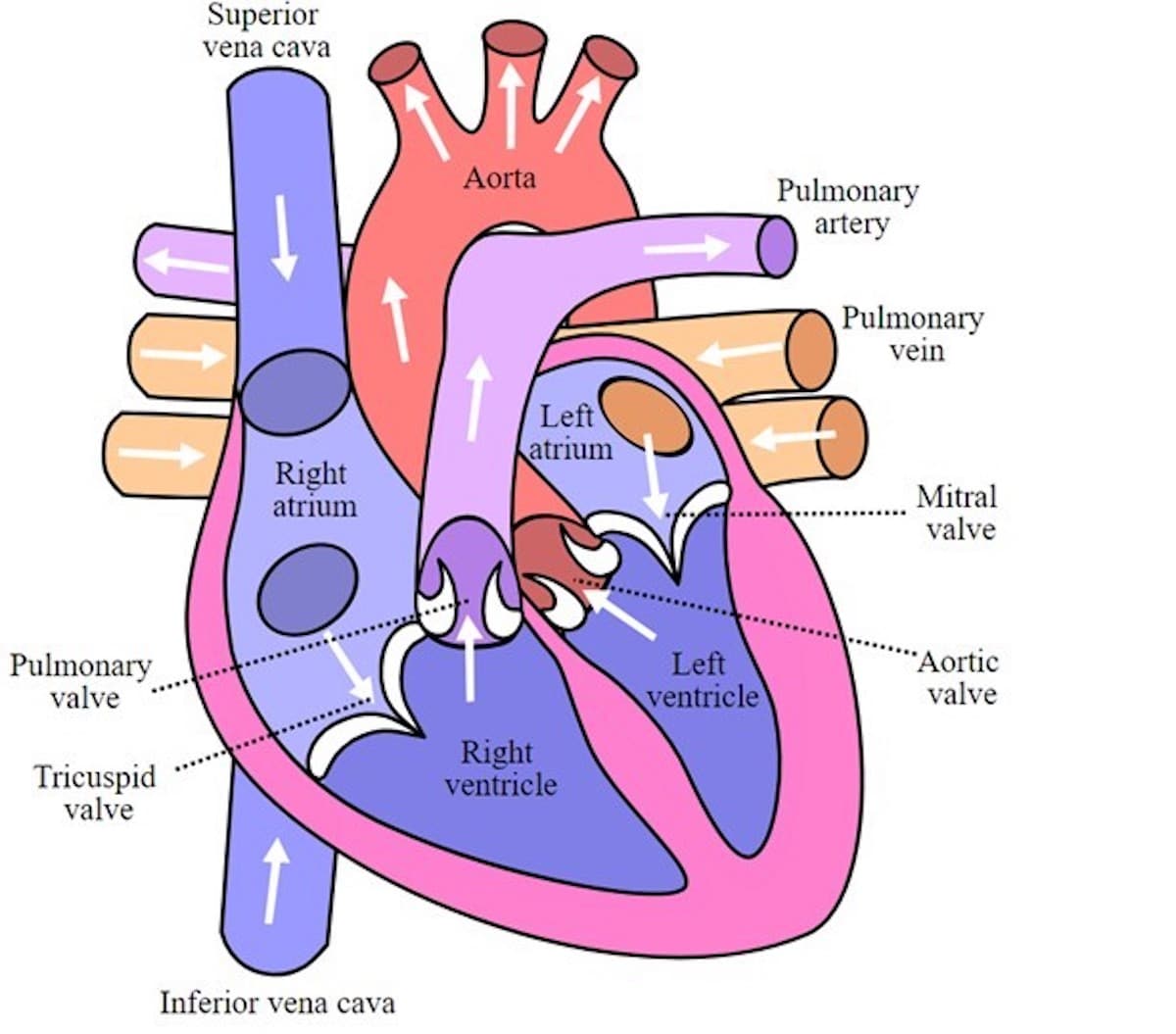
Credit: Wapcaplet, Yaddah, CC BY-SA 3.0 http://creativecommons.org/licenses/by-sa/3.0/, via Wikimedia Commons.
Deoxygenated blood enters the right side of the heart through two veins — the superior vena cava and the inferior vena cava. The superior vena cava brings deoxygenated blood from the upper body, and the inferior vena cava brings deoxygenated blood from the lower body. The deoxygenated blood from both veins enters the right atrium, which is the upper-right chamber of the heart. As the right atrium contracts, it pushes the deoxygenated blood through the tricuspid valve and into the right ventricle, which is the lower-right chamber of the heart. The purpose of these valves is to prevent the backflow of blood, ensuring that it flows in only one direction. Upon contraction of the right ventricle, deoxygenated blood is forced through the pulmonary valve and into the pulmonary artery, where it is carried away from the heart towards the lungs. In the lungs, the blood travels through the capillaries surrounding tiny air sacs called alveoli. Oxygen diffuses from the alveoli into the blood, while carbon dioxide moves from the blood into the alveoli for eventual exhalation.
The oxygenated blood from the lungs returns to the heart via four pulmonary veins and enters the left atrium. The left atrium contracts, pushing the oxygenated blood through the mitral valve into the left ventricle, the lower-left chamber of the heart. Forceful contraction of the left ventricle pumps the oxygenated blood through the aortic valve and into the aorta, the main artery of the body. The aorta carries the oxygenated blood away from the heart and distributes it to various organs and tissues throughout the body through small arteries, where it deposits oxygen and nutrients. As the oxygen is used up and waste products like carbon dioxide are produced, the blood becomes deoxygenated again and returns to the heart to repeat the cycle.
The State of the Fetal Lungs
What are the main differences between the circulatory system possessed by the infant (and adult), reviewed above, and that of the fetus in the uterus? Most importantly, the lungs are not yet active in gas exchange, and in fact are filled with fluid known as fetal lung fluid. This fluid helps the growth and development of the lungs, and also prevents the air sacs (alveoli) from collapsing due to the external pressure in the womb. Around the 24th to 28th week of gestation, the fetal lungs begin producing a substance called surfactant, a complex mixture of lipids and proteins that reduce surface tension in the alveoli, preventing them from collapsing during each breath. The production of surfactant is essential for the lungs to become functional after birth. The fetal lungs also contribute to the production and maintenance of amniotic fluid. As the fetus swallows amniotic fluid, some of it is taken up by the fetal lungs. This fluid is then processed and excreted back into the amniotic sac. This process helps in the development of the digestive and respiratory systems and maintains the appropriate volume of amniotic fluid for the fetus to move and grow.
Supplying the Fetus with Oxygen
Since the lungs are not active in gas exchange during pregnancy, how is the fetus supplied with oxygen? The fetus is connected to the mother’s circulatory system through the placenta, a specialized organ that forms inside the uterus and serves as the interface between the maternal and fetal blood supplies. Oxygen-rich blood from the mother’s circulatory system enters the placenta through the maternal arteries. The fetus’s blood and that of the mother never mix. The placenta contains numerous small blood vessels called villous capillaries, which have thin walls that allow for efficient gas exchange. Oxygen molecules diffuse from the maternal blood into the placental villous capillaries due to the concentration gradient. Once oxygen diffuses into the villous capillaries, it binds to hemoglobin in the fetal blood, causing the fetal blood to become oxygenated. The oxygenated blood from the placenta is carried back to the fetus through the umbilical vein, one of the three blood vessels present in the umbilical cord. The umbilical vein carries oxygenated blood rich in nutrients from the placenta to the fetal liver. A portion of the oxygenated blood in the umbilical vein bypasses the fetal liver through a short blood vessel called the ductus venosus. The ductus venosus directs this oxygenated blood to the inferior vena cava which carries blood to the right atrium of the fetal heart.
In the fetal heart, there is a temporary opening between the right and left atria called the foramen ovale. This opening allows a portion of the oxygenated blood from the right atrium to pass directly into the left atrium. By bypassing the non-functional fetal lungs, the foramen ovale helps to direct oxygenated blood to the rest of the body more efficiently. The oxygenated blood that flows into the right ventricle is pumped into the pulmonary artery. However, since the fetal lungs are non-functional, a shunt called the ductus arteriosus diverts this oxygenated blood away from the pulmonary circulation and directly into the descending aorta, which supplies oxygenated blood to the lower body. Deoxygenated blood from the fetal organs and tissues is collected in the two umbilical arteries, which carry it back to the placenta for reoxygenation and removal of waste products.
Changes in the Lungs
What changes must take place at birth to successfully make the switch from dependence upon the placenta to breathing air? The first major change pertains to the lungs, which remain collapsed and inactive until birth. The first breath that a baby takes after delivery triggers a series of physiological changes in the lungs, leading to the inflation of the alveoli and the initiation of respiratory function. As the baby passes through the birth canal, the chest is squeezed. This pressure change and compression of the chest help expel some of the fluid present in the airways and lungs. As the baby emerges into the outside world, there are significant changes in the level of carbon dioxide and oxygen in its bloodstream. During labor, the baby continues to receive oxygen from the mother’s placenta. After birth, however, the placental circulation is cut off, leading to a decrease in oxygen supply. This decrease in oxygen levels and the accumulation of carbon dioxide in the bloodstream are sensed by specialized chemoreceptors in the baby’s body. As the baby comes into contact with the cold air and the environment, its skin and nerve endings are stimulated, leading to reflexive responses, including gasping and taking the first breath. Stretch receptors in the lungs send signals to the brainstem, which, in turn, inhibits the respiratory centers that control breathing. This reflex prevents excessive expansion of the lungs and maintains proper lung function. If these stretch receptors fail, the result can be overinflation of the alveoli during inhalation, resulting in alveolar rupture and collapse.
As the lungs expand, the fetal lung fluid is pushed out, and absorbed or expelled from the baby’s airways. After birth, the fetal lung fluid is gradually cleared from the lungs and, with the help of surfactant, the lungs begin to perform the essential function of gas exchange. The transition from the non-functional fetal lung state to the fully functional adult lung state is one of the most crucial physiological changes that occur during the birth process.
Closure of the Foramen Ovale
As previously mentioned, there is a temporary opening between the right and left atria called the foramen ovale, which allows a portion of the oxygenated blood from the right atrium to pass directly into the left atrium, bypassing the nonfunctional fetal lungs. As the baby takes its first breath, the lung expansion and the increased oxygenation of the blood trigger changes in the pressure dynamics of the heart. The increased oxygenated blood returning from the lungs to the left atrium increases the left atrial pressure, while the reduced flow of deoxygenated blood from the body to the right atrium decreases the right atrial pressure. These changes in pressure cause the flexible tissue flap that covers the foramen ovale, known as the septum primum, to close the opening. The septum primum fuses with the septum secundum, a rigid membrane-like structure, effectively sealing the foramen ovale and creating a solid partition between the two atria. This separation prevents the mixing of oxygenated and deoxygenated blood, ensuring that all blood flows through the pulmonary circulation to be oxygenated by the lungs.
Closure of the Ductus Arteriosus
As described in the foregoing, the ductus arteriosus is a short blood vessel that connects the pulmonary artery to the descending aorta, bypassing the non-functional fetal lungs. This shunt allows a portion of the blood leaving the right ventricle to flow directly into the systemic circulation. After birth, as the baby takes its first breath and the lungs expand, the oxygen levels in the bloodstream increase significantly. The increased oxygen levels lead to the constriction and eventual closure of the ductus arteriosus. Within 12 to 24 hours following birth, the ductus arteriosus undergoes a process called functional closure, where the smooth muscle in the vessel wall contracts and closes off the passageway. Over the next two or three weeks, the ductus arteriosus undergoes permanent closure through fibrosis and eventually becomes a ligament called the ligamentum arteriosum.
The location of the foramen ovale and ductus arteriosus, and their state in the fetal and newborn heart respectively, are illustrated in the following figure.
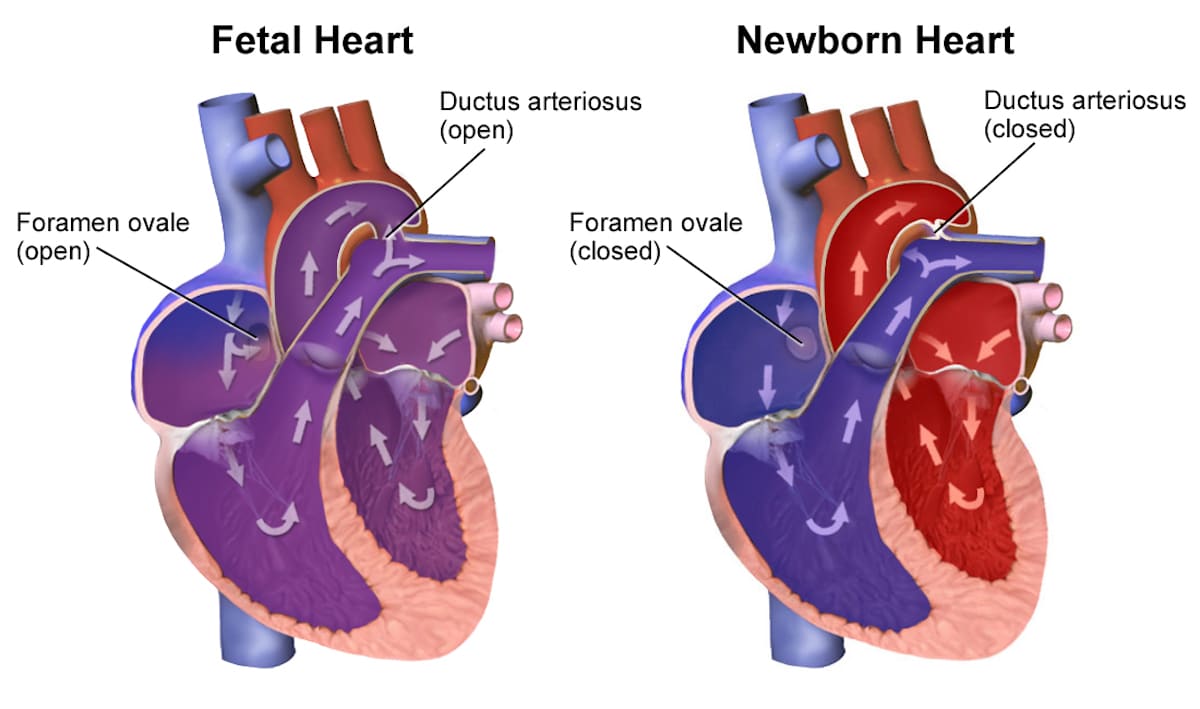
Credit: BruceBlaus, CC BY-SA 4.0 https://creativecommons.org/licenses/by-sa/4.0, via Wikimedia Commons.
Darwin or Design?
These changes in the lungs, valves, and vascular structures during the birth process are critical for the baby’s successful transition to the outside world and the establishment of a fully functional, non-shunted circulatory system. By effectively closing the foramen ovale and the ductus arteriosus, the baby’s heart and circulatory system are ready to assume the roles of efficient gas exchange through the lungs and the delivery of oxygenated blood to all organs and tissues, supporting the baby’s independent life outside the womb.
Medical physician Dr. David Galloway remarks [2],
Beyond the amazing physiology, we come to a second conundrum. Clearly a system like this has to work straight out of the blocks. If any significant component failed for whatever reason, anatomical anomaly, biochemical error or signaling failure, not only would the various changes be jeopardized, but the very survival of the newly-born infant would be seriously threatened. The amazing truth is that thousands of babies navigate this dangerous territory, every minute of every day. So, given our current understanding of the origin of complex systems in biology, how might such an exquisite arrangement have developed?
This is a good question, and it does seem to be quite implausible that such a system could have arisen through a trial-and-error step-wise process such as that envisioned by neo-Darwinian evolutionary theory. On the other hand, complex systems where multiple things have to work together simultaneously is precisely what we might expect on the supposition of design.
Footnotes
1. Galloway, D. Design Dissected — Is the Design Real? A Clinical Look at Life’s Complexity, Design, and Ultimate Causation (John Ritchie Publishing, 2021).
2. Ibid., 137-138.
1 thought on “The Genius of the Fetal Circulatory System”
Totally amazing! God is awesome and awe inspiring Thanks for the information.
Comments are closed.